Fluphenazine Decanoate vs Haloperidol Decanoate in Pregnancy: Which LAI Is Preferred?

Recently, we posted the following blog discussing the role of first-generation antipsychotics during pregnancy:
First-Generation Antipsychotics in Pregnancy: Still the Most Underrated Option?
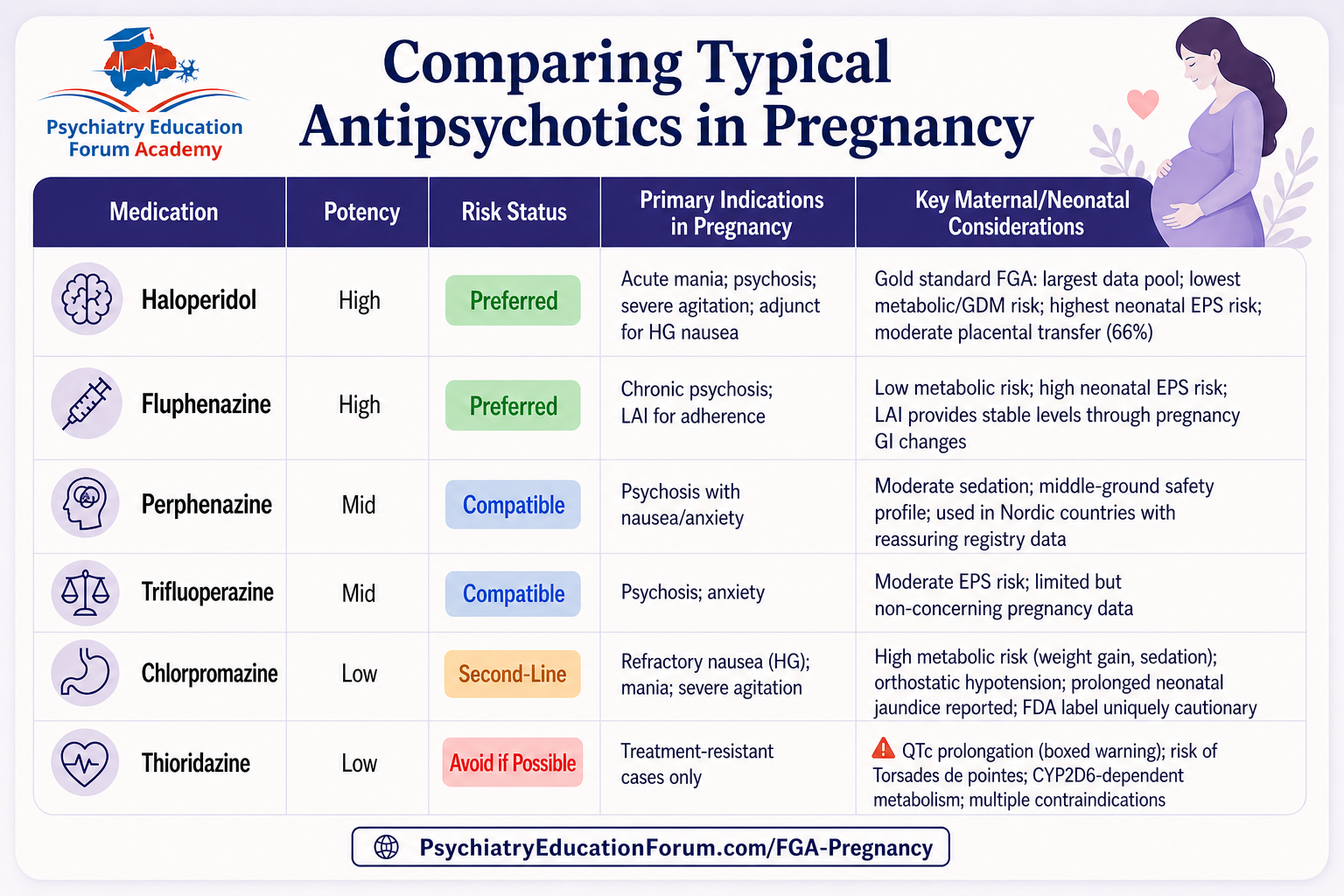
As part of that discussion, we shared the following comparison table highlighting the clinical positioning of several typical antipsychotics during pregnancy:
On our social media page, the following question was asked:
“Why fluphenazine instead of haloperidol for LAI?”
This blog post is the detailed answer to that question.
While second-generation antipsychotics are commonly discussed in modern practice, first-generation LAIs still retain an important role in carefully selected patients — particularly when adherence is a major concern.
Among the available first-generation LAIs, an important clinical question emerges:
Why might fluphenazine decanoate be preferred over haloperidol decanoate during pregnancy?
Below is a detailed review of the pharmacokinetic, metabolic, and clinical rationale behind this positioning. The following wording is intentionally preserved exactly as written for educational accuracy and discussion purposes.
1. The Core Advantage: Shorter Half-Life = Greater Clinical Flexibility
This is the most important reason.
- Fluphenazine decanoate has a significantly shorter apparent half-life than haloperidol decanoate — approximately 6.8–9.6 days after a single injection (extending to ~14.3 days at steady state), compared to haloperidol decanoate’s ~3 weeks (with steady-state not reached until 3–4 months). [1]
In pregnancy, this difference is critical because:
If the neonate develops EPS or withdrawal symptoms after delivery, fluphenazine will clear from the maternal (and therefore neonatal) system faster than haloperidol decanoate.
If a dose adjustment is needed due to pregnancy-related pharmacokinetic changes (plasma levels of haloperidol can drop by up to 52% in the third trimester), fluphenazine’s shorter half-life allows more responsive titration. [2]
The “lock-in” period — the time during which the drug cannot be removed if problems arise — is shorter with fluphenazine.
2. The Metabolic Advantage: Lower Weight Gain Risk
- The Lancet Psychiatry network meta-analysis of 18 antipsychotics ranked haloperidol as the best for weight (i.e., least weight gain), but this ranking was based on general population data. [3]
- In the FAERS disproportionality analysis, haloperidol actually had statistically significantly more weight increase reporting than many other antipsychotics — placing it alongside olanzapine and aripiprazole for weight gain signal. [4]
- Fluphenazine, by contrast, was not flagged for significant weight gain in the same analyses.
Pregnancy already imposes metabolic stress (gestational diabetes, weight gain, insulin resistance). For a pregnant woman already at risk for gestational diabetes and excessive weight gain, this distinction matters.
3. The Pharmacokinetic Stability Advantage: Bypassing GI Changes
This is the fundamental reason LAIs are considered during pregnancy in the first place.
- Pregnancy causes delayed gastric emptying, decreased GI motility, nausea/vomiting (especially in the first trimester), and altered intestinal absorption — all of which can reduce the bioavailability of oral antipsychotics unpredictably. [5-6]
- An LAI bypasses the GI tract entirely, providing stable, predictable serum levels regardless of nausea, vomiting, or hyperemesis gravidarum. [7-8]
- The table above in our last blog post, correctly identifies this as fluphenazine’s primary indication: “chronic psychosis; LAI for adherence” — meaning it is chosen specifically for patients where oral medication reliability is a concern.
Both haloperidol decanoate and fluphenazine decanoate share this advantage, but fluphenazine’s shorter half-life makes it the more maneuverable option during the dynamic pharmacokinetic environment of pregnancy.
4. The Dosing Flexibility Advantage
Fluphenazine decanoate can be administered at 2-, 3-, or 4-week intervals, providing greater dosing flexibility than haloperidol decanoate (which is standardized at 4-week intervals). [1][9]
In a double-blind trial comparing the two agents, the injection interval was stratified at 2, 3, or 4 weeks for fluphenazine, and the dosage equivalency was approximately 3:1 (haloperidol 75 mg : fluphenazine 25 mg). [9] This flexibility is valuable during pregnancy because:
As pregnancy progresses and drug clearance increases, the injection interval can be shortened (e.g., from every 4 weeks to every 3 weeks) to maintain therapeutic levels.
After delivery, when levels may rise due to the “postpartum level jump,” the interval can be lengthened or the dose reduced more nimbly.
5. The Congenital Malformation Signal: A Haloperidol-Specific Concern
- The WHO pharmacovigilance database analysis (131 million reports) found that haloperidol had a significantly higher reporting frequency for congenital malformations compared to quetiapine (ROR 3.83; 95% CI 2.62–5.59) — a signal not seen with other antipsychotics. [10]
- While causality is not established (and the FDA label notes that “causal relationships were not established” for reported limb malformations), this pharmacovigilance signal adds a layer of concern for first-trimester haloperidol exposure that does not exist for fluphenazine. [11-12]
- The network meta-analysis by Wang et al. (2025) similarly found that haloperidol did not show a statistically significant increase in congenital malformations (OR 1.26; 95% CrI 0.90–1.75), but the point estimate was higher than for several other agents. [13]
Summary: Why Fluphenazine LAI Over Haloperidol LAI in Pregnancy
| Factor | Fluphenazine Decanoate | Haloperidol Decanoate | Clinical Implication for Pregnancy |
|---|---|---|---|
| Apparent t½ | 6.8–14.3 days | ~3 weeks | Faster clearance if neonatal EPS occurs; more responsive dose titration |
| Dosing interval flexibility | 2, 3, or 4 weeks | 4 weeks (standard) | Can shorten interval as clearance increases in late pregnancy |
| Time to steady state | 4–6 weeks | 3–4 months | Faster achievement of therapeutic levels; faster washout if needed |
| Congenital malformation signal | No specific signal | ROR 3.83 vs. quetiapine (WHO database) | Haloperidol carries a pharmacovigilance signal not seen with fluphenazine |
| Metabolic/weight risk | Low | Low (but FAERS weight gain signal) | Fluphenazine may have a cleaner metabolic profile in pregnancy |
| GI bypass advantage | Yes (IM depot) | Yes (IM depot) | Both bypass pregnancy-related GI absorption changes |
Want the Full Clinical Framework?
This post gives you the overview.
But real clinical decision-making requires more than that.
Inside our Pregnancy & Breastfeeding Psychopharmacology: Rapid Decision Guide, every medication is broken down into a standardized, clinic-ready format:
- Executive summaries (rapid decision support)
- Teratogenicity and safety data
- Maternal vs fetal risk stratification
- Monitoring protocols
- Comparative tables across medications
- Patient counseling scripts
- EMR-ready documentation templates
- Clinical decision flowcharts
👉 And this FGA chapter is currently available as a FREE preview
🔗 Access below:
Explore the Full Series:
This is part of the Pregnancy & Breastfeeding Psychopharmacology series.
👉 View all upcoming chapters here:
Pregnancy & Breastfeeding Psychopharmacology
We continue to review and summarize clinically relevant research to support your daily practice.
INTERESTED IN ACCESS TO THIS & OTHER CLINICALLY RELEVANT LECTURE SERIES?
JOIN ACADEMY MEMBERSHIP
DISCOUNTS AVAILABLE FOR: Residents & Students ONLY.
Email us your student information (program information and way to confirm your student status) to: [email protected]
© 2026 All Rights Reserved.