Comparing Antipsychotics in Lactation: What Clinicians Need to Know
One of the most difficult conversations in perinatal psychiatry is not whether to treat illness during breastfeeding.
It is deciding which antipsychotic creates the best balance between:
- Maternal psychiatric stability
- Infant exposure risk
- Breastfeeding success
- Real-world clinical practicality
Unfortunately, most clinicians are forced to make these decisions using fragmented data, isolated case reports, and generalized recommendations that rarely address medication-specific differences.
That becomes especially important when considering dopamine partial agonists such as aripiprazole and brexpiprazole.
The Clinical Problem with Partial Agonists in Lactation
While medications like aripiprazole and brexpiprazole often have relatively low estimated infant exposure, the major concern is usually not direct infant toxicity.
The major concern is suppression of prolactin and reduction in milk supply.
Aripiprazole already has growing clinical concern regarding lactation failure, with some reports suggesting very high rates of breastfeeding disruption in susceptible patients.
Brexpiprazole appears pharmacologically similar enough that many clinicians are now approaching it with comparable caution — although direct lactation data remain extremely limited.
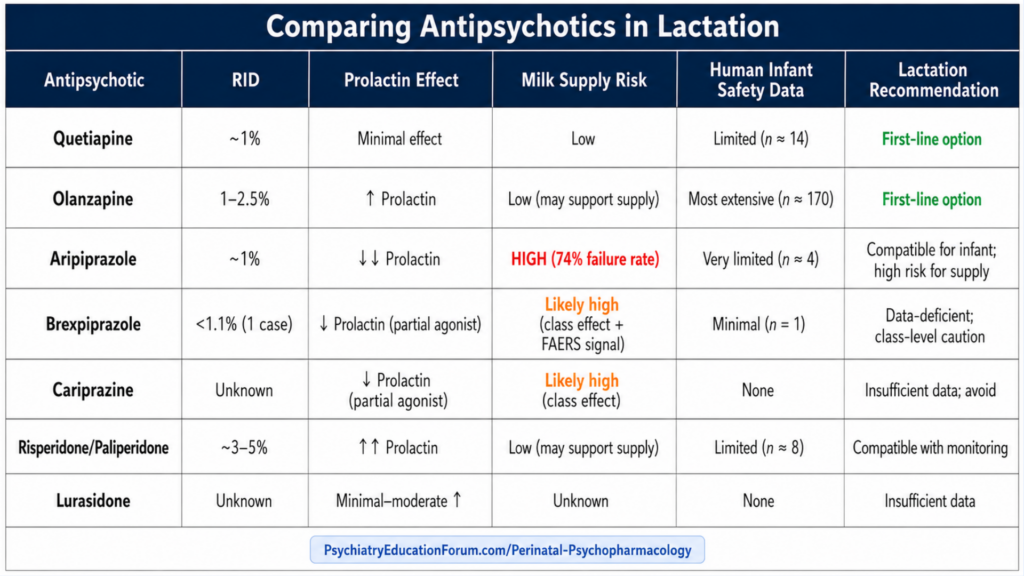
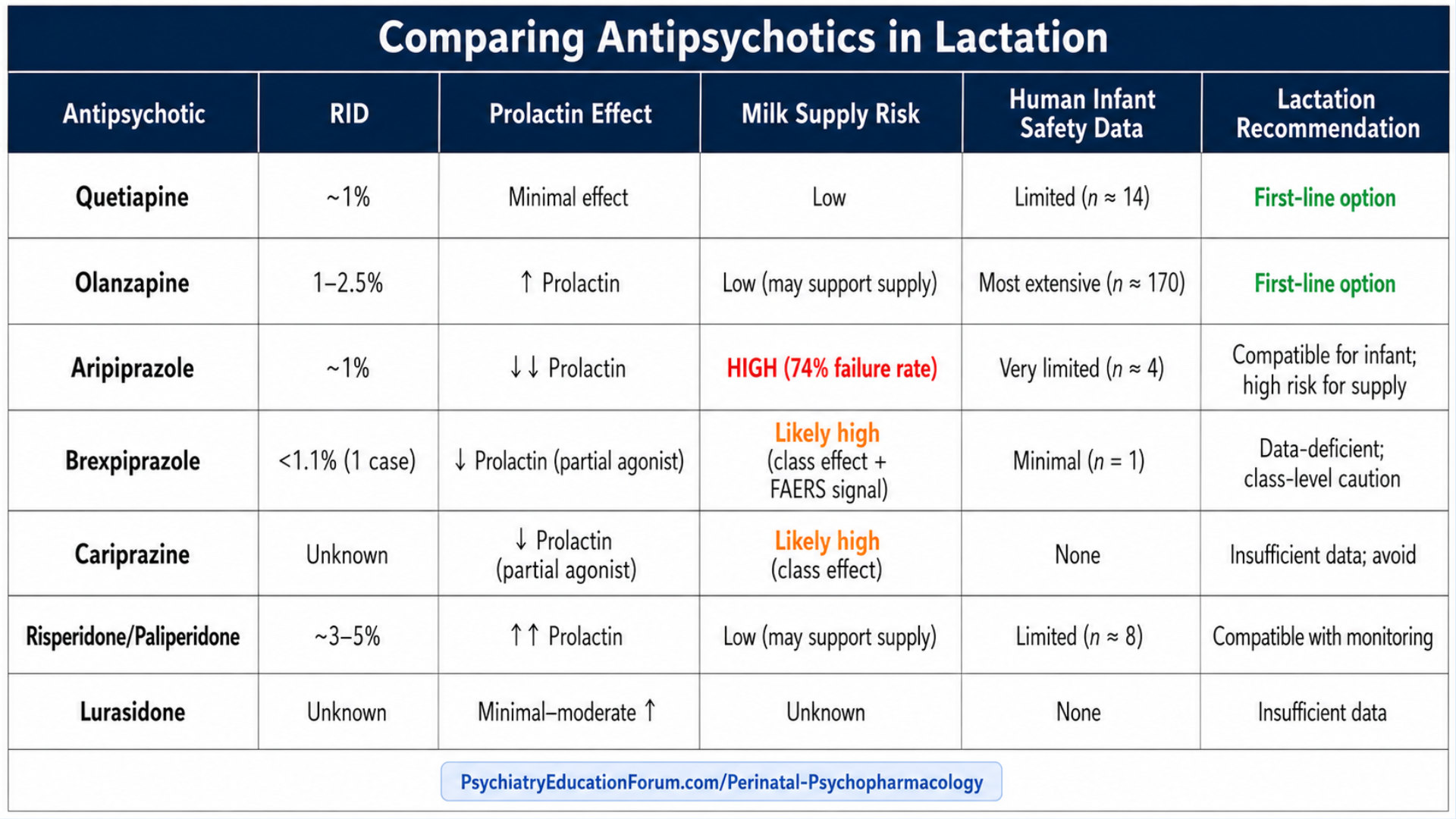
Comparative Positioning of Common SGAs During Breastfeeding
Key Clinical Takeaways
1. Low RID does not automatically mean “breastfeeding-friendly”
- A medication can have low infant exposure while still significantly impairing milk production. This is one of the biggest misconceptions in perinatal psychopharmacology.
2. Quetiapine and olanzapine remain the most clinically comfortable options
These agents currently have:
- The most reassuring breastfeeding experience
- Lower concern for lactation suppression
- Greater real-world clinician familiarity
3. Aripiprazole deserves more caution than many clinicians realize
- The prolactin-lowering effect may substantially impair breastfeeding success, even when infant exposure appears low.
4. Brexpiprazole remains highly data-deficient
- Current evidence is extremely limited. Until larger human lactation datasets emerge, many clinicians may prefer caution — especially in mothers strongly prioritizing breastfeeding success.
Start with a Free Preview:
Brexpiprazole use with Breastfeeding
Want the Full Clinical Framework?
This post gives you the overview.
But real clinical decision-making requires more than that.
Inside our Perinatal Psychopharmacology: Rapid Decision Guide, each Breastfeeding Chapter Is Structured for Rapid Clinical Decision-Making:
- Executive Summary – rapid, high-yield clinical takeaways for busy clinicians
- Lactational Pharmacology – RID, M/P ratio, oral bioavailability, protein binding, half-life, and milk transfer principles
- Human Lactation Data – exposed infant numbers, infant serum levels, and real-world breastfeeding outcomes
- Infant Safety & Monitoring – sedation, EPS, feeding issues, developmental considerations, and monitoring protocols
- Maternal Considerations – prolactin effects, milk supply impact, metabolic burden, sedation, and postpartum safety issues
- Formulation & Pharmacokinetic Considerations – oral vs LAI formulations, reversibility, dose timing, and postpartum level changes
- Comparative Clinical Positioning – preferred vs compatible vs high-caution agents and when to continue vs switch
- Drug-Specific Clinical Pearls – unique pharmacology, counseling nuances, and high-yield decision-making points
- High-Yield “Clinic-Ready” Tools – patient scripts, pediatrician communication templates, EMR documentation templates, and monitoring checklists
- Decision Algorithms – structured step-by-step guidance for real-world breastfeeding management scenarios
🔗 Access below:
Explore the Full Series:
This is part of the Pregnancy & Breastfeeding Psychopharmacology series.
👉 View all upcoming chapters here:
Perinatal Psychopharmacology
We continue to review and summarize clinically relevant research to support your daily practice.
INTERESTED IN ACCESS TO THIS & OTHER CLINICALLY RELEVANT LECTURE SERIES?
JOIN ACADEMY MEMBERSHIP
DISCOUNTS AVAILABLE FOR: Residents & Students ONLY.
Email us your student information (program information and way to confirm your student status) to: [email protected]
© 2026 All Rights Reserved.