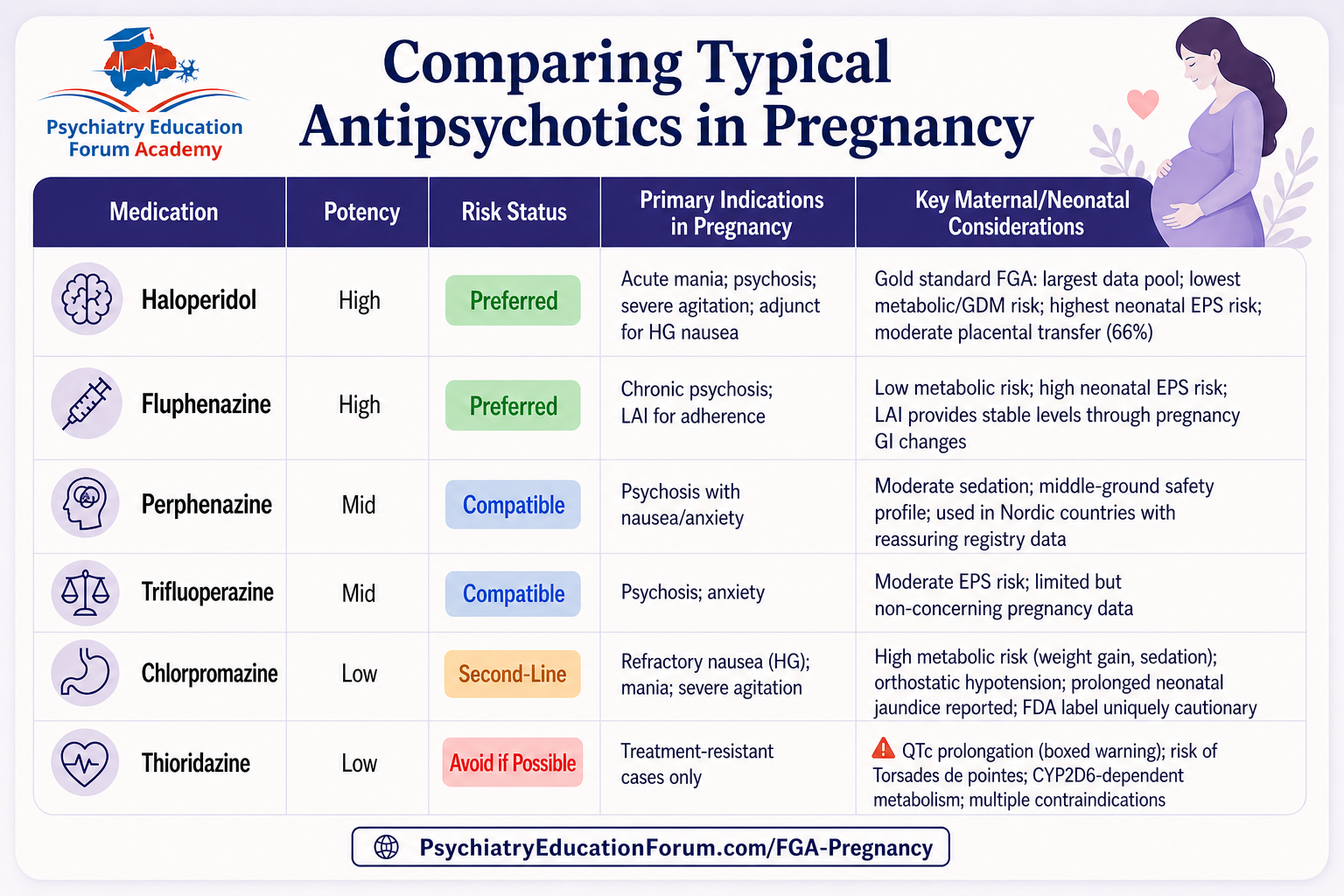
First-Generation Antipsychotics in Pregnancy: Still the Most Underrated Option?

Want the latest research insights delivered straight to your inbox? Subscribe to our Email Updates Here mailing list Psychedelic-assisted therapy (PAT) has been widely promoted…

Want the latest research insights delivered straight to your inbox? Subscribe to our Email Updates Here mailing list A newly published randomized clinical trial in…
PERINATAL PSYCHOPHARMACOLOGY Vortioxetine in Breastfeeding: A Unique Option for Postpartum Brain Fog? Understanding where vortioxetine fits when cognitive symptoms dominate postpartum depression Quick Take: Vortioxetine…

Want the latest research insights delivered straight to your inbox? Subscribe to our Email Updates Here mailing list A New Chemical Entity Built on Bioequivalence…

PERINATAL PSYCHOPHARMACOLOGY Should You Taper SSRIs Before Delivery? What the Data on PNAS Actually Says A practical, evidence-based approach to managing SSRI use near delivery—without…
Please confirm you want to block this member.
You will no longer be able to:
Please note: This action will also remove this member from your connections and send a report to the site admin. Please allow a few minutes for this process to complete.