Dr. Harvinder Singh
Forum Replies Created
-

Dr. Harvinder Singh
AdministratorJuly 26, 2021 at 2:05 pm in reply to: FACIAL EDEMA 2/2 ANTIPSYCHOTICS?Read our course chapter for more details on this topic:
-
Dr. Harvinder Singh
AdministratorJuly 20, 2021 at 4:44 pm in reply to: FACIAL EDEMA 2/2 ANTIPSYCHOTICS?My other thought is using the compounding pharmacy and working with them on creating sublingual formulations to avoid the risk of an allergic response from filler. I did that with 2 of my patient recently with good results except for the cost involved in this process.
-
Dr. Harvinder Singh
AdministratorJuly 20, 2021 at 3:01 pm in reply to: FACIAL EDEMA 2/2 ANTIPSYCHOTICS?Do check if you can get the genetic testing results: as you can check a specific polymorphism in one of the gene that increases the risk of side effects to serotonergic medications.
I will first start with getting a detailed history of side effects with each medication as getting edema with each medication trial is not making sense.
How about a trial of NAC as this has shown efficacy in reducing irritability for autism spectrum disorder.
-
Dr. Harvinder Singh
AdministratorJuly 19, 2021 at 6:38 pm in reply to: FACIAL EDEMA 2/2 ANTIPSYCHOTICS?Thanks for sharing this interesting case. Note that antipsychotic-induced edema is not an uncommon side-effect and can occur with any antipsychotic and any dose (risk is higher with a faster increase in medication). The most common site ie eyelid and face.
Case reports have shown the association of edema with the following antipsychotics:
- Risperidone
- Quetiapine
- Olanzapine
- Clozapine
- Ziprasidone
- Clozapine
- Amisulpride
The treatment recommendations are as follows:
- Avoid antipsychotics if possible.
- If an antipsychotic is chosen: change to different antipsychotics at low dose with slow titration: aripiprazole may be a good next option.
- I will consider medications in the following orders: antidepressants followed by lamotrigine, clonidine, guanfacine, and aripiprazole
- Get genetic testing to rule out the risk of slow metabolizers for certain medications.
- If she responds to certain antipsychotics and edema remains a limiting factor: the addition of a diuretic may be used as a last resort.
I will work on creating a separate chapter on this topic soon. Please keep us updated of your progress.
-
Dr. Harvinder Singh
AdministratorJuly 2, 2021 at 12:03 pm in reply to: How long to continue antipsychotic in bipolar after remission?Great job Mojahid & Fabiola.
Answer: 6 months.
Read this PEFA chapter for details: https://psychiatryeducationforum.com/lesson/antipsychotics-treatment-duration-after-mania-remission/
-
Hi Daramoon.
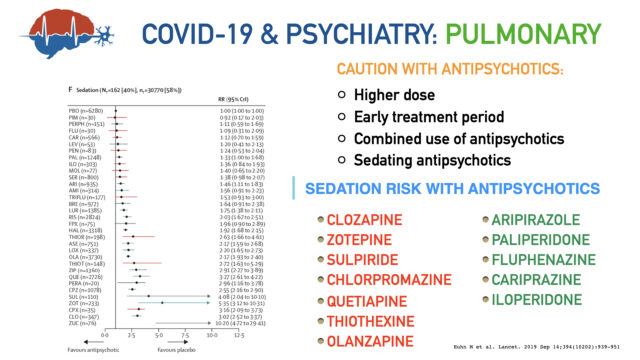
We have a whole section (with 5 chapters) dedicated to this topic of COVID-19 and Psychotropic medications:
https://psychiatryeducationforum.com/course/covid-19/
The choice of antipsychotics depends on the pulmonary risk (pneumonia), cardiac risk (QTc prolongation), hematologic risk, drug interactions, and other factors: watch all the chapters for more details).
I have attached a pic of one of the slide from the presentation on the use of antipsychotics with COVID19.
-
Dr. Harvinder Singh
AdministratorJune 14, 2021 at 7:18 am in reply to: PMDD Diagnosis: Must Symptoms?Answer: (c) Bloating/weight gain
Read our chapter for more details: https://psychiatryeducationforum.com/lesson/pmdd/
-
Hi Amelia. I agree with your plan of collaborating with sleep medicine before doing any changes.
Since patient is on higher Armodafinil dose of 500 mg (with max of 250 mg recommended for narcolepsy): I agree with tapering armodafinil and increasing methylphenidate (in collaboration with sleep medicine). This approach is safer compared to increasing methylphenidate on this high dose of armodafinil.
Keep us posted on the patient progress.
-
Dr. Harvinder Singh
AdministratorMay 31, 2021 at 9:35 am in reply to: stimulants and kidney disease -
Dr. Harvinder Singh
AdministratorMay 31, 2021 at 9:06 am in reply to: stimulants and kidney diseaseHi Amelia.
The “low dose” use of stimulants is safe in the elderly. I will stay cautious in patients with end-stage renal disease (by using lower doses) and not in patients with mild, moderate, or severe renal impairment. Read this study to learn more on this: PubMed.
Overall, low dose stimulants have shown efficacy in the following disorders in elderly:
- Geriatric depression secondary to medical illness: Dextroamphetamine (average maximal daily dose of 8.2 mg/day) and methylphenidate (maximal daily dose averaging 9mg/day).
- Post-stroke depression: Methylphenidate (mean dose of 17mg daily). read more on this topic here: Chapter
- Major depression resistant to other treatment: Methylphenidate (ranged between 5 and 20 mg daily)
- Apathy, Negative symptoms with dementia: Methylphenidate (ranging from 10 to 20 mg/day)
- Improving falls: Methylphenidate (10mg single dose)
The list is long. Let me know if you want me to post a chapter with a summary on this topic.
-
Dr. Harvinder Singh
AdministratorMay 28, 2021 at 8:15 am in reply to: Omega 3-Fatty Acids for Major Depressive DisorderAnswer: (f) None of the above.
All are correct options. Watch our journal club discussion for more details:
https://psychiatryeducationforum.com/lesson/journal-club-1/
This journal club will answer the following ten clinically relevant questions:
- Are omega-3 fatty acids effective as augmentation or as monotherapy for MDD management?
- What dose of omega-3 fatty acid is considered therapeutic for the treatment of MDD?
- What ratio of EPA/DHA is crucial for omega-3 fatty acids’s therapeutic benefit?
- Is pure EHA more efficacious than the combination of EHA/DHA for MDD?
- What is the recommended minimum duration of treatment with omega-3 fatty acid for the treatment of MDD?
- Is omega-3 fatty acid efficacious for recurrent depression?
- What are the common adverse events at the therapeutic dose of omega-3 fatty acid?
- What additional lab work is required when using the higher dosages of omega-3 fatty acid?
- How to ensure the omega-3 fatty acid’s product quality before buying?
- Do omega-3 fatty acid’s response in MDD have a relation with inflammatory biomarkers?
-
Dr. Harvinder Singh
AdministratorMay 16, 2021 at 11:54 am in reply to: DD between dual pathology VS. Substance induced mental illness?Hi Ahmed. I did the inpatient + consultation-liaison psychiatry work for 5 years before moving to outpatient psychiatry work now. It can be difficult to differentiate these two conditions initially and it can vary from 24 hr (in mild intoxication cases) to even 5 (or more) days for either high dose substance abuse or combined substance use. I never placed a timing on medical clearance for this reason and will always work with our medical unit colleagues to decide.
Our goal was to admit patients to the medical unit if:
- Unstable vitals, or
- need for multiple PRN medications to control the aggression, or
- abnormal labs (electrolytes, ammonia, or CPK levels)
I think building a good relationship with your medical unit physician is most important, as you can transfer them quickly in case patient is admitted first to psychiatry unit & they destabilized medically.
The question regarding the decision between admission to detoxification unit versus the acute psychiatric unit is similarly not the same for every patient. In these cases: admit to acute psychiatric unit only if patient is actively suicidal or at risk of self-harm or to others. Otherwise I don’t see any reasons to not do the detoxification first and then transfer to acute psychiatric unit if a patient is still having at-risk symptoms.
What criteria or guidelines you follow in your hospital.
-
Interesting question. I have not used Xyrem before but here are my thoughts:
- Stimulants are also the treatment of choice of narcolepsy: so you can target both narcolepsy and ADHD by using a stimulant unless your patient has severe cataplexy (where xyrem is known to be a good choice).
- The main side effect with Xyrem is excessive sedation & respiratory depression: but this side effect is mostly seen at higher doses or when combined with other sedating medications. Keep sertraline dosing for the late morning time or afternoon time to prevent any additive risk of sedation risk.
- Seizure is mentioned as a risk with abuse of Xyrem or when used with other CNS depressants: this will be my other worry with using Wellbutrin and Xyrem together.
- If this patient has a confirmed ADHD and narcolepsy diagnosis: switching Wellbutrin to stimulant will be my next choice before moving to Xyrem option.
Keep us updated on your decision and response. This will be agood learning experience for everyone.
-
Dr. Harvinder Singh
AdministratorJune 10, 2021 at 3:13 pm in reply to: Psychotropics & Risk of Tinnitus?Yes Bupropion is known to cause and should be avoided with history of tinnitus.
Watch the video lecture discussion (link below).
Here is one case report:
- Settle EC Jr. Tinnitus related to bupropion treatment. J Clin Psychiatry. 1991 Aug;52(8):352. (PMID: 1907965)
-
Dr. Harvinder Singh
AdministratorMay 13, 2021 at 7:15 pm in reply to: Difficult Case with Anxiety, Depression & Antidepressant Withdrawal.Most of her medication trials are limited due to the sedation side effects and stops them immediately despite multiple encouragement and education. I will keep lithium as an option if Lexapro followed by Buspirone augmentation is not helpful.
Her anxiety is more severe with panic attacks at this time compared to depression.