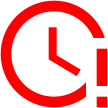
Severe Melancholic Depression: Diagnose & Treatment Options

Psychiatry Education Forum Academy is excited to announce the release of Academy’s 18th Journal Club Discussion: Anorexia Nervosa: How to Evaluate, Diagnose & Treat This…
Anorexia nervosa, a serious and potentially life-threatening eating disorder, goes far beyond its outward manifestation of extreme weight loss and food restriction. While the psychological…

We just finished our 13 journal club discussions at PEFA (Psychiatry Education Forum Academy). PEFA members can claim a maximum of 4.75 AMA PRA Category…
We begin PEFA Journal Club’s updated schedule with our first journal club discussion today: Journal Club #1: The Psychopharmacology Algorithm Project at the Harvard South…
Today we posted the following second journal club in PEFA Journal Club’s discussion series: Journal Club #2: International Society for Nutritional Psychiatry Research Practice Guidelines…
Please confirm you want to block this member.
You will no longer be able to:
Please note: This action will also remove this member from your connections and send a report to the site admin. Please allow a few minutes for this process to complete.